January 11,2022
M.sandhya
roll no 89
This is online E-blog, to discuss our patient de-identified health data shared after taking her guardian's signed informed consent.
Here we discuss our individual patient problems through series of inputs from available global online community of experts with an aim to solve the patients clinical problem with current best evidence based input.
This E-blog also reflects my patient's centred online learning portfolio.
I have been given this case to solve in an attempt to understand the topic of "Patient Clinical Data Analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with a diagnosis and treatment plan..
CASE SCENARIO:.
28 Year old male who is sales man by occupation presented to casualty complaints of
CHIEF COMPLAINTS
Seizures - 15 days
Fever with chills and rigors -10 days
Cough - 10 days.
HISTORY OF PRESENT ILLNESS:
Patient was apparently asymptomatic 11 months back then he noticed loss of weight about 10 kgs per month.
TIME LINE OF EVENTS:

Patient was apparently asymptomatic 11 months back , then he noticed rapid loss of weight which was about 10 kgs in a month
In the month of April,he went to a local hospital and after routine investigations found out his creatinine levels are high and diagnosed him with hypertension
He then went to a hospital in Hyderabad for confirmation and there he was told to start dialysis
Then on April 16 th ,he came to our hospital and was tested positive for COVID 19 and started on treatment.
From the month of April ,he was not going to work and stayed at home doing simple daily works .
Then he came to our hospital again in the month of June and had 28 dialysis sessions from June 24 th to September 19 th , regularly.
After that , he decided to remove central line and shift to AV fistula , which was failed once , then he tried again so was not on dialysis for 3 months( september to december)
•Then he had SEIZURES 15 days back , which was 3 episodes
each episode of seizure lasted for 3 to 5 minutes, associated with uprolling of eyeballs and frothing from mouth , there was post ictal confusion for about 30 minutes after 1st episode and about 10 to 15 minutes after 2nd and 3rd episode
Episode was not associated with biting of tongue and involuntary micturition
After 1st episode he was taken to nearby hospital for which he was admitted and treated for 3 days and then discharged.
After going to home ,he had 2 nd seizure episode at around 12 am ,which was for 3 -5 minutes , and then he had another 3 rd episodes at 3 am in the morning.
Then he came back to our hospital , again. he was started dialysis
-he also has complaints of shortness of breath ( Grade 2) which is insidious in onset and gradually progressive and aggravated more during lifting weights.
He also has cough since 10 days,not associated with sputum .
There was decreased urine output, and decreased appetite
chest pain since 10 days ,which was more during lying down flat
No history of burning micturition,red colour urine , nausea, vomiting, loose stools, head aches, confusion, dizziness
Patient was normal and shifted to ward ,but later he developed fever yesterday ,which is of high grade ,then he again was shifted to ICU .
PAST HISTORY :
•Known case of hypertension since 11 months
•Not a known case of diabetes, asthma, TB , any CHD
FAMILY HISTORY
no significant family history
PERSONAL HISTORY
▪Diet-mixed
▪ Appetite-decreased
▪Bowel movements-Regular
▪Bladder movements-Decreased since 10 days
▪Sleep adequate
▪Habits- he was alcoholic and stopped since 8 months, and not a smoker
GENERAL EXAMINATION
▪Patient is conscious , coherent and cooperative and well oriented to time place
and person, moderately built and moderately nourished
- Pallor- present
-Icterus-absent
-Cyanosis-absent
-Clubbing-absent
-Lymphadenopathy-absent
-Edema-absent
VITALS
Temperature-98.6
Pulse rate-88 bpm
Respiratory rate-14 cpm
BP-160/100 mm h
Spo2-98%
GRBS-130 mg%
SYSTEMIC EXAMINATION
▪CVS-- s1 ,s2 heard no murmurs
• Respiratory system- pleural rub heard on right side.
• Abdomen- no tenderness seen, no. . palpable mass seen, not distended
▪CNS-
-Patient is conscious
-Speech -normal
-No signs of meningeal irritation
-SENSORY EXAMINATION,- touch, pain , vibration present
-No muscle wasting seen
-Tone of muscles is normal
REFLEXES:
DEEP TENDON ;. Right. Left
KNEE JERK. +2. +2
ANKLE JERK. +2. +2
BICEPS. +2. +2
TRICEPS. +2. +2
SUPINATOR. +2. +2
•Power : Right. Left
BICEPS. +5. +5
TRICEPS. +5. +5
FLEXORS OF KNEE. +5. +5
EXTENSORS OF KNEE+5. +5
FLEXORS OF HIP. +5. +5
EXTENSORS OF HIP. +5. +5
•Gait -normal
▪Coordination
- Finger nose test-able to perform
- knee heel test- able to operform
- Romberg sign- negative
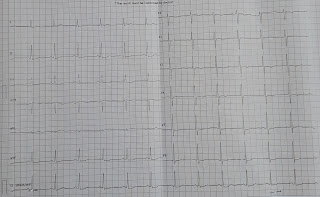
2d echo:
CBP:
HB : 5.6gm/dl
TLC: 4000cells/mm³
PLT: 1.99 lakh/mm³
ABG
PH: 7.12
PCO2: 13.1
HCO3:6.9
RFT
UREA : 239mg/dl
CREATININE : 16.8
URIC ACID : 16.8
CALCIUM : 8.2
Na+: 145
K+: 5.7
Cl- 107
LFT
ALT : 08
ALP : 164.
PROVISIONAL DIAGNOSIS:
UREMIC ENCEPHALOPATHY WITH CkD ON MHD WITH HYPERTENSIVE NEPHROPATHY.
TREATMENT:1) Fluid restriction( 1 ltr per day)
2)salt restriction( 2.4 g per day)
3)Tab NODOSIS( 550mg )PO/OD
4)Tab SHELCAL(500 mg) PO/OD
5)Tab OROFER Po/ OD..
6)Tab LASIX 40 mg PO / BD
7)TAB NICARDIA 10 mg PO/BD
















Comments
Post a Comment