80 year old female with SHORTNESS OF BREATH AND COUGH
80 year old female with SHORTNESS OF BREATH AND COUGH



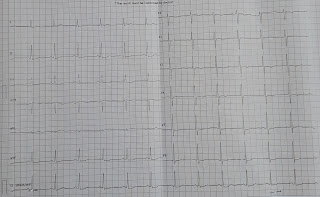
ECG
 2d echo
2d echo


June 6, 2022
M.sandhya
1701006117
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs. This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment box
80 year old female who is dailywaged labour by occupation and came to opd with
CHIEF COMPLAINTS;
shortness of breath since 10 days
dry cough since 3 days
HISTORY OF PRESENT ILLNESS;
Patient was apparently asymptomatic 20 yrs back then
she had history of giddiness and headache for which she went to hospital and diagnosed with hypertension and from then on regular medication Currently using Tab. Atenolol 50mg + Amlodipine 5mg once daily.
6 yrs back she had history of polyuria for which she went to RMP who told her that she had uncontrolled sugars and prescribed Tab.metformin 500 mg once daily.
3 yrs back she had history of pain abdomen and diagnosed with appendicitis and appendicectomy was done
2 yrs back she had shortness of breath initially on exertion and later progressed to even at rest associated with pedal edema and bilateral plueral effusion diagnosed with left lower lobe collapse with acute cardiogenic pulmonary edema then
2D echo showing dilated right and left atria ,concentric LVH ,moderate PAH.
Since then patient had no symptom
10 days back she developed shortness of breath ,which is insidious in onset gradually progressive from exertion to rest since 3 days associated with dry cough.
Dry cough- non productive,non foul smelling.since 3 days.
PAST HISTORY;
Known case of Diabetes and hypertension.
Underwent appendicectomy - 3 yrs back.
Has a history of similar complaints in the past .
FAMILY HISTORY:-
insignificant
PERSONAL HISTORY:-
DIET-mixed
APEPTITE- Normal
BOWEL &BLADDER-Regular
SLEEP-Adequate.
ADDICTIONS- Alcohol monthly twice (2-3yrsback).
GENERAL EXAMINATION:-
Patient is conscious, coherent,cooperative.
Well oriented to time place & person
Moderate built and moderately nourished.
Pallor present
No cyanosis, clubbing, icterus, LN
Vitals :
Bp -140/70 mmhg
PR -48 bpm ;irregularly irregular
RR : 20 cpm
Spo2 : 84 on RA, 96 On 4lts O2

SYSTEMIC EXAMINATION :
CARDIOVASCULAR SYSTEM:-
Inspection-
Chest is elliptical and bilaterally symmetrical
no raised jvp
Apical impulse present.
No engorged veins.
Palpation-
Inspectory findings are confirmed .
No- thrills, rubs.
Apex beat -2cms lateral to mid clavicular line.
Percussion-
Right and left heart borders normal.
Auscultation-
S1 S2 heard
No murmurs.
RESPIRATORY SYSTEM:-
Dyspnea- present
No wheeze
Breath sounds - vesicular
No Adventitious sounds
ABDOMINAL EXAMINATION:-
No tenderness
No palpable liver and spleen.
Bowel sounds - present.
CENTRAL NERVOUS SYSTEM:-
Higher mental function- intact
No- meningeal signs.
Normal - cranial nerves
Normal- motor and sensory system.
No- abnormal reflexes.
INVESTIGATIONS:-
PREVIOUS- 18-06-2020
chest X-ray


ECG
#PROVISIONAL DIAGNOSIS:-
HEART FAILURE WITH PRESERVED EJECTION FRACTION
WITH CARDIOGENIC PULMONARY EDEMA.
TREATMENT:-
1)Inj. Atropine 0.5ml/iv/sos
2)Inj.pantop.40mg/iv/OD
3)Inj.lasix 40mg /iv/bd( 8:00am & 4:00pm)
4)Inj. Zofer 4mg /iv/sos
5)Tab .Ecosporin -Av 75/10mg/OD
6)Inj.CLEXANE 60mg/sc
7)Tab.OROFER-XT po/OD
Comments
Post a Comment